Abstract
Paternal feeding and child care are significant determinants of child nutrition, health, and well-being. In many Kenyan communities, fathers seldom participate; child care is predominantly perceived as the mother's responsibility. Limited paternal involvement may negatively impact the quality of child nutrition and care in the home. This study investigated fathers’ roles, perceptions, and barriers to participation in child feeding and care in Kathonzweni Ward, Makueni County, Kenya. The study used an exploratory qualitative design. Researchers conducted 11 focus group discussions with fathers, mothers, and community health promoters to understand paternal practices, perceptions, and challenges. They audio-recorded, transcribed, and thematically analyzed each session to find key themes. Five main themes emerged: paternal roles (financial support and direct care), effects of paternal involvement on child health, barriers, cultural norms and evolving practices, and support needs. Fathers mostly provided financial support and decided on household food and health costs; a few helped with daily feeding and care. Younger and more educated fathers were more likely to feed, play with, and take children to health facilities. Economic hardship, substance use, limited nutrition knowledge, and prevailing gender norms constrained fathers’ participation. Further, societal and cultural beliefs that caregiving constitutes women’s work discouraged male involvement. Nevertheless, most participants agreed that children benefited from paternal involvement through improved nutrition, health, and family cohesion. The study urges sharing caregiving and feeding tasks equally between parents. Recommendations include health education for men, community awareness, and livelihood support to empower fathers as caregivers. Involving men in maternal and child health and removing social barriers can normalize their participation. These strategies could improve child nutrition and well-being in rural Kenya.
Keywords
Paternal Involvement, Child Feeding, Caregiving, Gender Norms, Nutrition
1. Introduction
Healthy feeding habits in childhood are crucial for survival, growth, and cognitive development, as they prevent chronic diseases later in life
| [1] | Hollis, J. L., Collins, C. E., DeClerck, F., Chai, L. K., McColl, K., & Demaio, A. R. (2020). Defining healthy and sustainable diets for infants, children and adolescents. Global Food Security, 27, 100401. |
[1].
Infant deaths often relate to malnutrition, with Sub-Saharan Africa (SSA) accounting for over a third of these deaths
. In addition, fewer than half of SSA children aged 6-23 months receive adequate meals, emphasizing the need to strengthen household feeding practices to improve child nutrition .
A growing body of literature has emphasized the importance of fathers in infant and young child feeding (IYCF) and care. Fathers contribute not only through financial provision but also by offering emotional support, participating in decision-making, and engaging in caregiving tasks. Research in SSA has revealed that paternal engagement in feeding is associated with improved dietary diversity and nutritional status among children aged 6-23 months
| [4] | Bolka, A., Assaye, M., & Phliphos, A. (2025). Male Partner Involvement in Child Feeding and Associated Factors Among Children Aged 6 to 23 Months in Hawassa City, Sidama Region, Southern Ethiopia: A Community Based Cross Sectional Study. Food Science & Nutrition, 13(7), e70557. |
[4]
. Conversely, limited paternal involvement is correlated with malnutrition, particularly in one-parent or female-headed households
| [5] | Seifu, B. L., Asebe, H. A., Fente, B. M., Melkam, M., Asmare, Z. A., Asnake, A. A.,... & Negussie, Y. M. (2025). The effect of maternal high-risk fertility behavior on child nutritional status in Sub-Saharan Africa: a propensity score-matched analysis. Frontiers in Public Health, 13, 1512392. |
[5].
In Kenya, disparities in child nutrition have been rising, with increasing malnutrition among children aged 6-23 months. Stunting rates exceed 30 percent in counties such as West Pokot, Kilifi, Samburu, and Garissa. In Makueni County, 20 percent of children under five are stunted, 9 percent are underweight, and 4 percent are wasted, with malnutrition more prevalent in rural areas
. Frequent droughts, water shortages, and limited access to health services cultural and social beliefs about childcare, exacerbate these trends
. In many communities, including Kathonzweni Ward, fathers are viewed primarily as breadwinners, while mothers assume the responsibility for feeding and daily childcare. These entrenched gender norms often restrict men’s participation, hindering efforts to improve child nutrition outcomes.
To further situate this study, it draws on theoretical perspectives from gender and masculinity studies, which help explain how cultural expectations shape men’s caregiving roles. Connell’s (1995) concept of
hegemonic masculinity highlights how dominant gender norms position caregiving as a feminine domain, discouraging men from engaging in domestic or nurturing roles
. However, emerging frameworks such as gender-transformative approaches by
| [17] | Barker, L. A., Gout, B. S., & Crowe, T. C. (2011). Hospital Malnutrition: prevalence, identification and impact on patients and the healthcare system. International Journal of Environmental Research and Public Health, 8(2), 514-527. https://doi.org/10.3390/ijerph8020514 |
| [18] | Cardona-Morrell, M., Prgomet, M., Lake, R., Nicholson, M., Harrison, R., Long, J., Westbrook, J., Braithwaite, J., & Hillman, K. (2015). Vital signs monitoring and nurse-patient interaction: A qualitative observational study of hospital practice. International Journal of Nursing Studies, 56, 9-16. https://doi.org/10.1016/j.ijnurstu.2015.12.007 |
[17, 18]
illustrate a gradual redefinition of fatherhood, one that promotes shared caregiving, empathy, and partnership between men and women. These perspectives provide a useful analytical lens for understanding how fathers in Makueni County negotiate traditional expectations while increasingly taking on active roles in feeding and childcare.
This research paper, therefore, investigates how fathers contribute to the feeding and care of children between 6-23 months in Makueni County, particularly in Kathonzweni Ward. It explores how cultural practices and community perceptions shape fathers' participation in feeding and childcare. The study incorporates the perspectives of fathers, mothers, and community health promoters. Findings reveal that while fathers acknowledge the importance of involvement in childcare, cultural norms and economic pressures continue to limit their participation. The paper concludes that tailored community sensitization and universal nutrition education are essential to promoting more balanced parental roles and improving child health.
2. Materials and Methods
2.1. Study Area
This research was done in Kathonzweni Ward, Makueni County, southeast of Kenya. The county is located in the arid and semi-arid regions of Kenya (ASALs) and is marked by its uniqueness in agroecological zones, unpredictable rainfalls, frequent droughts, and chronic food insecurity
. The significant sources of livelihood include small-scale crop production, livestock farming, and informal employment. The undernutrition problem in children under five years old is still relevant despite a wide range of health and nutrition programs due to the lack of dietary diversity and inefficient childcare
The ward was intentionally chosen due to its unique agro-ecological zones, diverse rural livelihoods, susceptibility to malnutrition, and the perceivable disparity in the paternal involvement in the infant and young child feeding (IYCF).
2.2. Study Design and Participants
To gain an in-depth understanding of the role of paternal feeding and child care among families with children aged 6-23 months, an exploratory qualitative design was used. This qualitative method was suitable to address the complexity of gendered practices and the socio-cultural context that manipulates paternal engagement
| [9] | Creswell, J. W. and Poth, C. N. (2018) Qualitative Inquiry and Research Design Choosing among Five Approaches. 4th Edition, SAGE Publications, Inc., Thousand Oaks. |
[9]
. It was done on fathers, mothers, and the Community Health Promoters (CHPs) who offer regular health and nutrition counselling. Fathers and mothers were engaged in disaggregated Focus Group Discussions (FGDs) by age (<30 years and >30 years) so that they could freely talk and minimize social desirability bias. Conversely, CHPs attended Key Informant Interviews (KIIs) to give a professional opinion of the community-level practices.
2.3. Sampling Methods
The respondents were chosen using purposive sampling, being the primary caregivers (father and mother) of a child 6-23 months old, from households with father-mother-child triad representation. The FGDs consisted of 8-10 participants, which was sufficient to have the group dynamics. The recruitment was performed in partnership with the village health committees and local health facilities that helped in the selection of the eligible fathers and mothers with children between the ages of 6-23 months and had lived in the region for at least one year. CHPs were chosen due to their experience in promoting maternal and child health and nutrition in communities. Recruitment and data collection were done to the point of thematic saturation.
2.4. Data Collection Procedures
Semi-structured FGD guides in which the essential thematic areas were identified, such as paternal involvement in feeding and care, issues faced, cultural factors, and perceived effects on child nutrition, were used to collect data. The guides were also created in English and translated into Kikamba, the most commonly used local language, and translated back to maintain uniformity. All the sessions were conducted in neutral community settings by trained facilitators who knew both languages to maximize privacy and comfort. The discussions took 45-90 minutes each, and these were recorded on tape, with the consent of participants, and with copious field notes. The facilitators used probing and reflective questions to bring out detailed answers, especially from the young participants or those who were less articulate.
Qualitative analysis, particularly FGDs, was chosen deliberately because they encourage collective reflection on shared norms and practices. This is very valuable when exploring cultural expectations and community perceptions of gender roles. FGDs allow participants to build on each other’s experiences and reveal normative pressures that shape paternal behaviour, which may be less visible in individual interviews
2.5. Data Management and Analysis
All audio recordings were transcribed word-for-word and translated into English. Thematic analysis of data was conducted according to the six-step. Framework by
: familiarization, first codes generation, theme search, theme review, defining and naming themes, and generating the final report. The coding method was predominantly inductive, where patterns were developed when participants were narrating their stories. NVivo software for qualitative data analysis helped in the systematization of codes and the retrieval of pertinent pieces of text. The investigator triangulation, peer debriefing, and member checking of a subset of the participants helped to increase the credibility of the study by confirming the accuracy of the emerging interpretations.
2.6. Ethical Considerations
NACOSTI gave ethical approval, and the research permission was granted by Makueni County Department of Health Services. The research followed the ethics principles as stipulated in the Declaration of Helsinki (World Medical Association, 2013). All the participants provided informed consent upon the precise determination of the study aims, voluntary involvement, and the guarantee of confidentiality. Participants were made aware of the fact that they could withdraw at any point, and they were also given pseudonyms to ensure that their identity was not compromised when the data was transcribed and reported.
3. Results
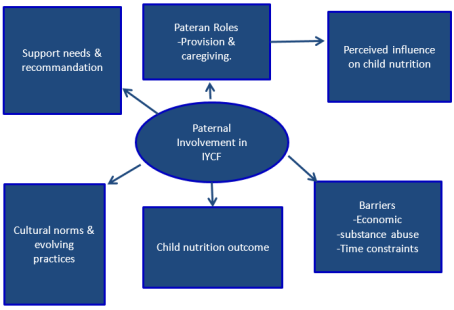
A total of 11 focus group discussions were conducted, with fathers (<30 years and ≥30 years), mothers (<30 years and ≥30 years) in groups as to their age, and community health promoters (CHPs). Group sizes ranged between eight and ten participants, and discussions lasted 45-90 minutes. Thematic analysis yielded five major themes: (1) Paternal Roles (provision and financial support, direct caregiving practices) (2) perceived influence of paternal involvement on child health and wellbeing, (3) barriers to paternal participation, (4) cultural norms and evolving practices, and (5) support needs and recommendations.
Table 1. Summary of Focus Group Discussions Conducted.Summary of Focus Group Discussions Conducted.Summary of Focus Group Discussions Conducted.
Category of Participants | Age Group | Number FGDs | Participants per FGD | Total Participants |
Fathers | < 30 years | 2 | 8-10 | 18 |
Fathers | ≥ 30 years | 2 | 8-10 | 18 |
Mothers | < 30 years | 2 | 8-10 | 18 |
Mothers | ≥ 30 years | 2 | 8-10 | 18 |
Community Health Promoters (CHPs) | Mixed age group | 3 | 8-10 | 27 |
Paternal Roles
a. Provision and Financial Support
The majority of participants across all groups identified financial provision as the main paternal contribution to child feeding and care. Fathers were described as providers responsible for ensuring food availability and other household necessities. As one CHP observed, "In this community, the father's duty is to ensure food is available; he provides money, and the mother takes care of cooking and feeding" (CHP6, FGD3).
Furthermore, most fathers described their role as financial support for mothers to buy food and child necessities e.g., diapers/napkins, a statement supported by several mothers who noted that men who lack stable jobs occasionally sold livestock or casual labor earnings to offer support. A younger father explained, "I make sure my wife has money for food so that our baby can eat and she can breastfeed well by doing all manner of jobs" (Father <30, FGD1). Although considered essential, this form of support was widely viewed as the limit of male involvement in child feeding and care.
b. Direct Caregiving Practices
About half of the younger fathers (<30 years) and a few older fathers reported engaging in direct caregiving activities such as feeding, bathing, comforting the child when distressed, and playing with their children. Mothers and CHPs confirmed that such involvement, while not the norm, is gradually increasing among the younger generation. "Some men are starting to feed and play with their children; you see it more with the younger fathers who have gone to school," explained a CHP (CHP5, FGD2). However, it was acknowledged that such support is only common when the mother is away or engaged somewhere.
A middle-aged father described, "When my wife goes to the market, I feed and bathe the baby. It is not every day, but I can do it when needed" (Father <30, FGD3). Despite this progress, most fathers acknowledged that their caregiving involvement remains occasional, primarily when mothers are unavailable.
c. Perceived Influence of Paternal Involvement on Child Health and Well-being
Nearly all groups linked greater paternal involvement, both financial and hands-on, to improved child nutrition, health, and emotional development. CHPs and mothers agreed that when fathers provide adequate resources or share caregiving duties, children are healthier, more energetic, and gain weight faster. "Children with supportive fathers are stronger and happier; they eat better," stated one CHP (CHP 4, FGD1).
A mother of a one-year-old child added, "When my husband helps to feed the baby, I feel less stressed, and the child eats more" (Mother <30, FGD2). Fathers also believed that active participation builds family unity and reduces maternal fatigue.
d. Barriers to Paternal Involvement
Across all focus group discussions, economic hardship consistently emerged as the most dominant barrier limiting fathers' engagement in child feeding and care. Unemployment and irregular income were repeatedly mentioned as constraints that reduced men's ability to provide food and participate in caregiving activities. As one young father explained, "You cannot help much when you have no job. Even staying home with the child feels like failure because you are supposed to be out looking for work" (Father 5, Father >30, FGD2). This economic pressure often forces fathers to prioritize income-generating activities over time spent with their children.
Alcohol and drug use were also highlighted, particularly by CHPs and mothers, as key impediments to consistent paternal involvement. A good number of participants observed that substance use among some young fathers drains limited household resources and contributes to neglect of family responsibilities. "Some men spend what little they earn on alcohol and drugs, forgetting their families" (CHP3, FGD3). This behavior not only weakens the fathers' financial support role but also leads to tension within households.
Additionally, long and inflexible working hours, especially among casual laborers and transport workers, were cited as significant time-related constraints. One mother observed, "My husband leaves before sunrise and returns late at night. The baby is usually asleep by the time he gets home" (Mother 6, Mother >30, FGD2). This highlights the challenge of balancing livelihood demands with caregiving duties in low-income rural settings.
e. Cultural Norms and Evolving Practices
Cultural expectations were identified as a significant structural barrier shaping gendered caregiving roles. The majority of participants agreed that caregiving tasks, such as feeding, bathing, cooking, and general nurturing, are traditionally perceived as women's work. One older father explained, "Other men laugh at a man who cooks or feeds a baby. Our fathers never did that" (Father 4, father >30, FGD2).
Nevertheless, signs of cultural transition were evident. Roughly half of CHPs and mothers reported noticing a slow but steady shift among younger, educated fathers who are more willing to participate. As one CHP observed, "Young men now see caring for their children as love, not weakness. It is changing slowly" (CHP8, FGD1). Exposure to health education sessions and church-based teachings was said to be influencing this gradual transformation.
f. Support Needs and Recommendations
Participants proposed various strategies to strengthen paternal participation in child feeding and care. About three-quarters of respondents recommended community-based sensitization and education programs specifically targeting men through barazas, churches, and health facilities. A CHP emphasized, "If fathers are taught about feeding and child care the same way mothers are, they will take part more" (CHP7, FGD2).
In addition, livelihood interventions, including job creation and income-generating activities, were also viewed as essential to reduce the economic burden that limits fathers' involvement. Finally, a few participants advocated for male-friendly health services and peer father support groups to encourage sharing of experiences and learning.
4. Discussion
The results show that Kathonzweni Ward fathers remain mostly described financial providers. This trend positions the majority of domestic contributions to child feeding as financial, as opposed to physical caregiving. This provider-centered pattern is based on the historical gender norms that have been recorded in Kenyan and other sub-Saharan literature
| [11] | Kaloro, K., Mahlelehlele, B., & Turkson, R. K. D. (2024). Fathers Role in Infant Feeding and Care: Exploring perceptions, practices, and challenges in Lesotho’s rural communities. Research Square (Research Square). https://doi.org/10.21203/rs.3.rs-5326825/v1 |
[11]
and contributes to the explanation of why most paternal inputs are not always associated with the improvement of feeding habits. The qualitative descriptions of this paper indicate that financial provision, although necessary, is not a complete channel to improved child nutrition since it does not guarantee proper intra-household resource allocation, responsive feeding, and prompt care-seeking. These empirical impressions are in line with household bargaining and ecological models, where the resources intertwine with caregiving behavior to produce nutrition outcomes.
In line with the provider discourse, there is substantial evidence of growing direct caregiving in paternity among a group of younger and better-educated men. There are cases of fathers who feed, bathe, and play with young children, although still occurrences indicate the shifting masculinities and changing parenting identities. These changes are consistent with the research that shows that exposure to education, health communication, and other role models may soften strict gendered divisions of care
| [12] | Mmari, K., Simon, C., & Verma, R. (2024). Gender-Transformative interventions for young adolescents: What have we learned and where should we go? Journal of Adolescent Health, 75(4), S62-S80. https://doi.org/10.1016/j.jadohealth.2024.04.016 |
| [13] | Olgay, S. Ş., Kırık, B., Uğur, E., & Özkan, H. A. (2025). From classroom to clinic: a qualitative study of gendered experiences among nursing students and educators in Türkiye. BMC Nursing, 24(1). https://doi.org/10.1186/s12912-025-03648-y |
[12, 13]
. The positive effects witnessed when fathers play an active role are significant because they underscore the indirect causal mechanisms by which paternal intervention can add to the maternal caregiving resources, and thus, improve child well-being.
Furthermore, respondents consistently reported a favorable association between paternal involvement and the physical and psychosocial development of children. Reports among mothers whose children's fathers were engaged in child care and feeding, families had more unity, and children had positive developmental and nutritional outcomes
| [14] | Jeong, J., McCann, J. K., Bhojani, A., Maguet, Z., Uyehara, M., & Ochieng, M. (2024). Fathers’ engagement in a parenting program primarily intended for female caregivers: An early qualitative process evaluation in Western Kenya. PLOS Global Public Health, 4(10), e0003520. https://doi.org/10.1371/journal.pgph.0003520 |
[14].
Although these qualitative perceptions are not causal, they do reveal probable processes, direct food provisioning, feeding assistance, and emotional/psychosocial support to the mother, which should be quantitatively tested. This analytic research must henceforth be aimed at measuring these pathways and determining their individual relative impact on the anthropometrical and developmental outcomes.
The most salient barriers to paternal participation were identified as economic hardship, substance abuse, and time constraints. The ubiquitous nature of livelihood insecurity implies that a lot of fathers focus on generating income, at the cost of presence and participation in day-to-day childcare. Alcohol, miraa locally known as “
muguka’, substance abuse was again and again pointed out as a waste of resources and a weakened paternal role. Such behavioural and structural limitations reflect the results of other East African settings, where economic precarity and male out-migration narrow father-child engagement
| [14] | Jeong, J., McCann, J. K., Bhojani, A., Maguet, Z., Uyehara, M., & Ochieng, M. (2024). Fathers’ engagement in a parenting program primarily intended for female caregivers: An early qualitative process evaluation in Western Kenya. PLOS Global Public Health, 4(10), e0003520. https://doi.org/10.1371/journal.pgph.0003520 |
[14]
. The solutions to these interconnected issues will involve interventions that decrease economic vulnerability and risk factors at the same time.
The cultural norms are at the center of determining who does what in the home. The shame of men doing sensitive, caring duties (diapering or bathing female children) was also a common motif and embodies more profound constructions of masculinity that promote nurturing as feminizing. Ethnographic and programmatic data indicate that these norms are difficult to change, but changeable; discussions at a community level, a combination of role models, and positive messages can shift caregiving as a complement to, rather than conflicting with, masculinity
| [15] | Zarzycki, M., Seddon, D., Bei, E., Dekel, R., & Morrison, V. (2022). How Culture Shapes informal Caregiver Motivations: A Meta-Ethnographic Review. Qualitative Health Research, 32(10), 1574-1589. https://doi.org/10.1177/10497323221110356 |
[15]
. The reported gradual change among younger men in Kathonzweni who are increasingly defining caregiving as an act of love and responsibility is thus essential, as it provides a demonstration of a viable point of normative intervention.
The participation recommendations are consistent within three strategic areas: economic empowerment, male-targeted behaviour change communication, and health system adaptations. Income-generation activities and livelihood support were regarded as preconditions to meaningful father engagement. Meanwhile, male-based community spaces (churches, markets, barazas) sensitization was accepted as a good way to reach people. A low-cost solution to enhance paternal knowledge and involvement is the integration of father-focused modules into regular health contacts, e.g., couple counseling during antenatal and growth-monitoring visits. Because substance abuse was so prevalent in the data, a combination of livelihood and psychosocial and addiction support could produce synergetic effects on child nutrition and family functioning.
Altogether, the qualitative data in Kathonzweni Ward make fathers an untapped yet potentially effective source of enhancing early childhood nutrition and wellbeing. The programming required will have to be multi-component, in which structural constraints are considered, and normative as well as behaviour change is encouraged. Through the combination of economic assistance, focused education, and community-focused normative intervention, policymakers and practitioners can develop enabling conditions in which fathers will transition beyond the stage of provision to active and long-term caregiving relationships that can benefit children, mothers, and households as well.
Implication of the Policy and Practice
The results of this research have significant implications for the policies of the Kenyan and the Sub-Saharan African communities on issues related to health and nutrition policies. The strategy to strengthen paternal involvement in infant and young children feeding (IYCF) needs interventions that target the cultural and structural barriers to male participation.
To start with, gender-transformative methods, including fathers, must be employed by nutrition and health promotion programs, which invalidates the traditional view that fathers should not engage in child feeding, since it is always a maternal responsibility. Shared caregiving responsibilities can be normalized by incorporating men in community nutrition education sessions, growth monitoring, and behavior change communication.
Second, community health volunteers and extension workers need training on involving both parents during home visits and outreach. Male attendance should be encouraged in antenatal and postnatal clinics to strengthen both male and female roles in child nutrition and care.
Third, policy documents like the Kenya National Nutrition Action Plan (2023-2027) and county health plans must clearly identify men as key in child health initiatives. This recognition will support the creation of family-based care models that incorporate fathers into regular maternal and child health programs.
Lastly, sensitization of the populations using the local media, religious organizations, and community groups can be instrumental in changing the social norms regarding fatherhood. Such campaigns can shift the culture of masculinity and caregiving with time by showing good examples of male caregivers, which will help in changing the culture.
Innovation and contribution
This study provides nuanced, context-specific evidence on the evolving nature of paternal practices in rural Kenya. It captures both the persistence of traditional provider roles and the emerging hands-on caregiving engagement among younger fathers. The findings highlight a critical yet underexplored opportunity: fathers represent an effective but often overlooked pathway for improving child nutrition and overall household well-being. By foregrounding men's roles in infant and young child feeding, the study advances understanding of gendered care dynamics and offers actionable insights for program design. The evidence points to the need for targeted strategies that address economic barriers, challenge entrenched gender norms, and strengthen fathers' caregiving competencies to promote equitable parenting and enhance nutritional outcomes.
Strengths and limitations
Key strengths of this research include the purposive sampling of father-mother-child triads, which ensured diverse family perspectives. Age-segmented focus group discussions minimized social desirability bias, while the use of local language with back-translation enhanced clarity and validity. Thematic analysis was systematic and supported by investigator triangulation and participant validation. However, the study relied on self-reported behaviours and perceptions, limiting causal inference. Its focus on a single ward may also restrict broader generalization. Future mixed-methods studies should quantify the relationship between paternal involvement, child anthropometric measures, and developmental outcomes to deepen and validate these findings.
Figure 1. Thematic framework of paternal involvement in IYCF.
5. Conclusions
This paper discussed the roles, perceptions and beliefs of fathers in feeding and care their children in Kathonzweni Ward, Makueni County. Their results highlight that even though fathers still remain largely seen as economic providers, there are emerging trends that indicate that there is progressive change in the way young and more educated men have been more direct caregivers. This change, even though marginalized, means the changing gender regulations that can improve the child nutrition and family wellbeing in general. The findings show that paternal engagement has a positive impact on the child's feeding outcomes, not only by providing financial aid but also by lessening maternal workload, enhancing emotional well-being, and promoting more regular feeding and care routines. These observations confirm the fact that paternal effects in ensuring effective involvement go beyond the income given to the family to the caregiving, physical and decision-making involvement.
Nevertheless, the ongoing socio-economic challenges, especially poverty, unemployment, and drug abuse, still stand in the way of men's involvement and desire to engage in childcare. Strong cultural beliefs that stigmatize male care providers add to this issue and help to solidify genderized divisions of responsibility. These barriers have to be dealt with in a dual approach that involves a combination of normative change and structural empowerment. Policy and programmatic approaches must therefore consider incorporating father-focused interventions in the current nutrition and health models, which should involve the provision of inclusive education, economic empowerment, and behaviour change communication. Caregiving can also be redefined as a positive part of good fatherhood through community discussions and male mentorship programs. In addition, the integration of psychosocial assistance and addiction recovery into livelihood initiatives will enhance the level of family stability and increase the success of child feeding.
Finally, the paper makes an important observation that fathers are an underexploited but vital resource in enhancing child nutritional status in rural Kenyan contexts. Multi-sectoral collaboration, which entails the connection of health, social protection, and community development mechanisms, will be crucial in ensuring sustainable development, as men will be given incentives to play meaningful roles in care and feeding their children. The perception changes that have been observed gradually, although clearly in Kathonzweni Ward, are also an indication of a good platform that can be used to develop interventions that will bring equitable and holistic caregiving in families.
Abbreviations
FGDS | Focus Group Discussions |
IYCF | Infant and Young Child Feeding |
CHP | Community Health Promoter |
SSA | Sub-Saharan Africa |
Acknowledgments
I sincerely appreciate the invaluable guidance and support provided by Prof. Judith Kimiywe and Dr. Juliana Kiio throughout the research process. Gratitude is also extended to the research assistants and statistician for their contribution to data collection and analysis. Special thanks go to the National Commission for Science, Technology, and Innovation (NACOSTI) and the Makueni County Government for granting research authorization. The assistance of the Community Health Assistant, Kathonzweni Ward, and all Community Health Promoters who participated in household identification and data collection is highly acknowledged. Lastly, sincere appreciation is extended to all caregivers who voluntarily participated in this study.
Funding
The authors received no financial support for conducting the research and for the publication of this article.
Conflicts of Interest
The authors declare that they have no conflict of interest.
References
| [1] |
Hollis, J. L., Collins, C. E., DeClerck, F., Chai, L. K., McColl, K., & Demaio, A. R. (2020). Defining healthy and sustainable diets for infants, children and adolescents. Global Food Security, 27, 100401.
|
| [2] |
World Health Organization. (2023). Infant and young child feeding. WHO.
https://www.who.int/news-room/fact-sheets/detail/infant-and-young-child-feeding
|
| [3] |
Raley, S., Bianchi, S. M., & Wang, W. (2012). When do fathers care? Mothers’ economic contribution and fathers’ involvement in child care. American Journal of Sociology, 117(5), 1422-1459.
https://doi.org/10.1086/663354
|
| [4] |
Bolka, A., Assaye, M., & Phliphos, A. (2025). Male Partner Involvement in Child Feeding and Associated Factors Among Children Aged 6 to 23 Months in Hawassa City, Sidama Region, Southern Ethiopia: A Community Based Cross Sectional Study. Food Science & Nutrition, 13(7), e70557.
|
| [5] |
Seifu, B. L., Asebe, H. A., Fente, B. M., Melkam, M., Asmare, Z. A., Asnake, A. A.,... & Negussie, Y. M. (2025). The effect of maternal high-risk fertility behavior on child nutritional status in Sub-Saharan Africa: a propensity score-matched analysis. Frontiers in Public Health, 13, 1512392.
|
| [6] |
Kenya National Bureau of Statistics. (2023). Kenya National Information Platform for Food and Nutrition: An analysis of the national progress and household characteristics associated with stunting (March 2021).
https://www.knbs.or.ke/wp-content/uploads/2023/09/Kenya-National-Information-Platform-For-Food-And-Nutrition-An-Analysis-Of-The-National-Progress-And-Household-Characteristics-Associated-With-Stunting.pdf
|
| [7] |
Republic of Kenya. (2022). Makueni County climate risk assessment report. Government of Kenya.
https://makueni.go.ke/sandbox/site/files/2024/06/Makueni-County -Pdf
|
| [8] |
UNICEF. (2023, June 6). “infant and young child feeding”. UNICEF DATA.
https://data.unicef.org/topic/nutrition/infant-and-young-child-feeding/#:~:text=Ideally%2C%20infants%20should%20be%20put,semi%2Dsolid%20and%20soft%20foods
|
| [9] |
Creswell, J. W. and Poth, C. N. (2018) Qualitative Inquiry and Research Design Choosing among Five Approaches. 4th Edition, SAGE Publications, Inc., Thousand Oaks.
|
| [10] |
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77-101.
https://doi.org/10.1191/1478088706qp063oa
|
| [11] |
Kaloro, K., Mahlelehlele, B., & Turkson, R. K. D. (2024). Fathers Role in Infant Feeding and Care: Exploring perceptions, practices, and challenges in Lesotho’s rural communities. Research Square (Research Square).
https://doi.org/10.21203/rs.3.rs-5326825/v1
|
| [12] |
Mmari, K., Simon, C., & Verma, R. (2024). Gender-Transformative interventions for young adolescents: What have we learned and where should we go? Journal of Adolescent Health, 75(4), S62-S80.
https://doi.org/10.1016/j.jadohealth.2024.04.016
|
| [13] |
Olgay, S. Ş., Kırık, B., Uğur, E., & Özkan, H. A. (2025). From classroom to clinic: a qualitative study of gendered experiences among nursing students and educators in Türkiye. BMC Nursing, 24(1).
https://doi.org/10.1186/s12912-025-03648-y
|
| [14] |
Jeong, J., McCann, J. K., Bhojani, A., Maguet, Z., Uyehara, M., & Ochieng, M. (2024). Fathers’ engagement in a parenting program primarily intended for female caregivers: An early qualitative process evaluation in Western Kenya. PLOS Global Public Health, 4(10), e0003520.
https://doi.org/10.1371/journal.pgph.0003520
|
| [15] |
Zarzycki, M., Seddon, D., Bei, E., Dekel, R., & Morrison, V. (2022). How Culture Shapes informal Caregiver Motivations: A Meta-Ethnographic Review. Qualitative Health Research, 32(10), 1574-1589.
https://doi.org/10.1177/10497323221110356
|
| [16] |
Holter, Ø. G. (1996). Book reviews: R. W. Connell: Masculinities. Cambridge: Polity Press, 1995. Acta Sociologica, 39(3), 337-341.
https://doi.org/10.1177/000169939603900309
|
| [17] |
Barker, L. A., Gout, B. S., & Crowe, T. C. (2011). Hospital Malnutrition: prevalence, identification and impact on patients and the healthcare system. International Journal of Environmental Research and Public Health, 8(2), 514-527.
https://doi.org/10.3390/ijerph8020514
|
| [18] |
Cardona-Morrell, M., Prgomet, M., Lake, R., Nicholson, M., Harrison, R., Long, J., Westbrook, J., Braithwaite, J., & Hillman, K. (2015). Vital signs monitoring and nurse-patient interaction: A qualitative observational study of hospital practice. International Journal of Nursing Studies, 56, 9-16.
https://doi.org/10.1016/j.ijnurstu.2015.12.007
|
Cite This Article
-
APA Style
Muinde, N., Kimiywe, J., Kiio, J. (2025). Paternal Role on Feeding and Childcare: Exploring Practices, Perceptions and Challenges in Makueni County; A Qualitative Study. Journal of Food and Nutrition Sciences, 13(6), 326-333. https://doi.org/10.11648/j.jfns.20251306.13
 Copy
|
Copy
|
 Download
Download
ACS Style
Muinde, N.; Kimiywe, J.; Kiio, J. Paternal Role on Feeding and Childcare: Exploring Practices, Perceptions and Challenges in Makueni County; A Qualitative Study. J. Food Nutr. Sci. 2025, 13(6), 326-333. doi: 10.11648/j.jfns.20251306.13
Copy
|
Download
AMA Style
Muinde N, Kimiywe J, Kiio J. Paternal Role on Feeding and Childcare: Exploring Practices, Perceptions and Challenges in Makueni County; A Qualitative Study. J Food Nutr Sci. 2025;13(6):326-333. doi: 10.11648/j.jfns.20251306.13
Copy
|
Download
-
@article{10.11648/j.jfns.20251306.13,
author = {Neema Muinde and Judith Kimiywe and Juliana Kiio},
title = {Paternal Role on Feeding and Childcare: Exploring Practices, Perceptions and Challenges in Makueni County; A Qualitative Study
},
journal = {Journal of Food and Nutrition Sciences},
volume = {13},
number = {6},
pages = {326-333},
doi = {10.11648/j.jfns.20251306.13},
url = {https://doi.org/10.11648/j.jfns.20251306.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.jfns.20251306.13},
abstract = {Paternal feeding and child care are significant determinants of child nutrition, health, and well-being. In many Kenyan communities, fathers seldom participate; child care is predominantly perceived as the mother's responsibility. Limited paternal involvement may negatively impact the quality of child nutrition and care in the home. This study investigated fathers’ roles, perceptions, and barriers to participation in child feeding and care in Kathonzweni Ward, Makueni County, Kenya. The study used an exploratory qualitative design. Researchers conducted 11 focus group discussions with fathers, mothers, and community health promoters to understand paternal practices, perceptions, and challenges. They audio-recorded, transcribed, and thematically analyzed each session to find key themes. Five main themes emerged: paternal roles (financial support and direct care), effects of paternal involvement on child health, barriers, cultural norms and evolving practices, and support needs. Fathers mostly provided financial support and decided on household food and health costs; a few helped with daily feeding and care. Younger and more educated fathers were more likely to feed, play with, and take children to health facilities. Economic hardship, substance use, limited nutrition knowledge, and prevailing gender norms constrained fathers’ participation. Further, societal and cultural beliefs that caregiving constitutes women’s work discouraged male involvement. Nevertheless, most participants agreed that children benefited from paternal involvement through improved nutrition, health, and family cohesion. The study urges sharing caregiving and feeding tasks equally between parents. Recommendations include health education for men, community awareness, and livelihood support to empower fathers as caregivers. Involving men in maternal and child health and removing social barriers can normalize their participation. These strategies could improve child nutrition and well-being in rural Kenya.
},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Paternal Role on Feeding and Childcare: Exploring Practices, Perceptions and Challenges in Makueni County; A Qualitative Study
AU - Neema Muinde
AU - Judith Kimiywe
AU - Juliana Kiio
Y1 - 2025/11/28
PY - 2025
N1 - https://doi.org/10.11648/j.jfns.20251306.13
DO - 10.11648/j.jfns.20251306.13
T2 - Journal of Food and Nutrition Sciences
JF - Journal of Food and Nutrition Sciences
JO - Journal of Food and Nutrition Sciences
SP - 326
EP - 333
PB - Science Publishing Group
SN - 2330-7293
UR - https://doi.org/10.11648/j.jfns.20251306.13
AB - Paternal feeding and child care are significant determinants of child nutrition, health, and well-being. In many Kenyan communities, fathers seldom participate; child care is predominantly perceived as the mother's responsibility. Limited paternal involvement may negatively impact the quality of child nutrition and care in the home. This study investigated fathers’ roles, perceptions, and barriers to participation in child feeding and care in Kathonzweni Ward, Makueni County, Kenya. The study used an exploratory qualitative design. Researchers conducted 11 focus group discussions with fathers, mothers, and community health promoters to understand paternal practices, perceptions, and challenges. They audio-recorded, transcribed, and thematically analyzed each session to find key themes. Five main themes emerged: paternal roles (financial support and direct care), effects of paternal involvement on child health, barriers, cultural norms and evolving practices, and support needs. Fathers mostly provided financial support and decided on household food and health costs; a few helped with daily feeding and care. Younger and more educated fathers were more likely to feed, play with, and take children to health facilities. Economic hardship, substance use, limited nutrition knowledge, and prevailing gender norms constrained fathers’ participation. Further, societal and cultural beliefs that caregiving constitutes women’s work discouraged male involvement. Nevertheless, most participants agreed that children benefited from paternal involvement through improved nutrition, health, and family cohesion. The study urges sharing caregiving and feeding tasks equally between parents. Recommendations include health education for men, community awareness, and livelihood support to empower fathers as caregivers. Involving men in maternal and child health and removing social barriers can normalize their participation. These strategies could improve child nutrition and well-being in rural Kenya.
VL - 13
IS - 6
ER -
Copy
|
Download